FT. LAUDERDALE, FL., October 15, 2015– Neil Spector, MD knows cancer. As a leading researcher, he led the development of two targeted cancer therapies which were FDA approved. He is currently the Sandra Coates Chair in Breast Cancer Research at Duke University. But in 2009, Dr. Spector faced his own mortality when a physician informed him he would die without a heart transplant. Dr. Spector’s heart had been destroyed by an undiagnosed case of Lyme disease.
Dr. Spector discussed his experiences as an oncologist and Lyme disease survivor on Friday, October 16, 2015 at the ILADS conference held at the Marriott Harbor Beach Resort in Fr. Lauderdale, Florida. His presentation was titled: How Lessons from Personalized Cancer Care Can Inform Management of Lyme Disease.
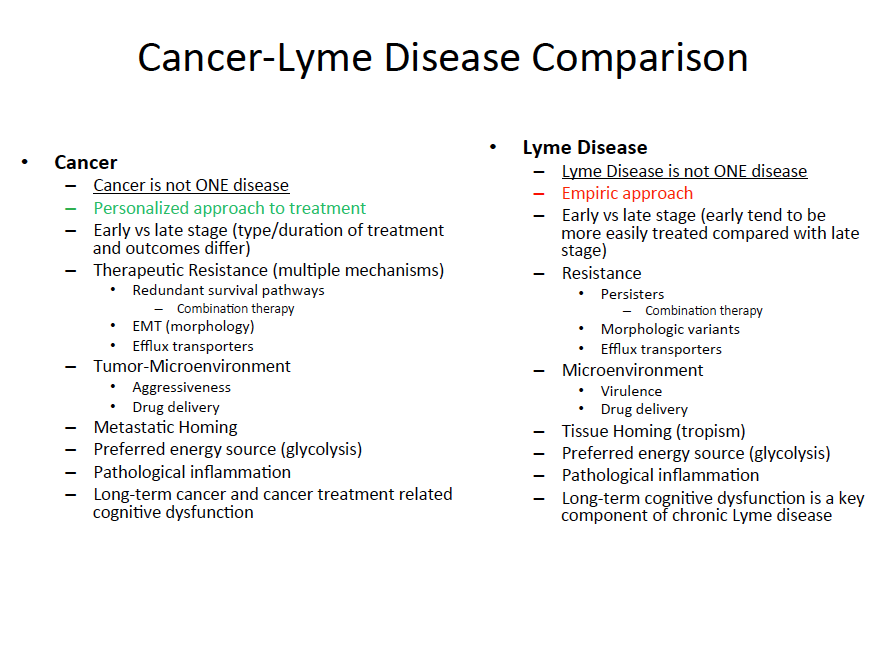
Dr. Spector calls Lyme disease “the infectious disease equivalent of cancer.” Cancer is not one specific disease and neither is Lyme, says Spector. “We talk about Lyme Disease as if it is ONE disease caused by one uniform strain of Borrelia when we know there are at least 16 pathogenic strains of the bacteria that cause disease in the United States.”
Spector notes both cancer cells and Borrelia burdoferi (the spirochete which causes Lyme disease) are equipped with mechanisms to resist therapeutic interventions. Both pathogens have a “sweet tooth,” says Spector, since each relies on glucose as a source of energy. Yet, while cancer specialists design personalized treatment plans for cancer patients, Lyme disease treatments are generally still one-size-fits-all.
“We have all witnessed via the media the struggles of Yolanda Foster and Avril Lavigne,” says Spector. They publicly put a face on the private suffering of many Lyme patients, and this suffering is a direct result of a lack of understanding about Lyme and its co-infections,” he says.
In a talk before the International Lyme and Associated Diseases Society (ILADS), Spector called for more “out-of-the-box thinking” on how to diagnose and treat Lyme disease and its co-infections.
“I am not taking sides in this debate,” says Spector. “As a patient and physician-scientist involved in cancer research and drug development, I have a unique perspective on the way Lyme disease is currently diagnosed and treated, and the gaps in our understanding of the disease beg for more research funding.”
A slide from Dr Spector’s presentation at ILADS
To clarify the slide the “green” personalized approach to treatment is where the treatment of Lyme Disease NEEDS to be but currently IS NOT. Instead, Lyme Disease is treated empirically (red), which is less scientifically based.
More research and research dollars are desperately needed to change this current state!!”
Dr Spector’s presentation at the ILADS conference can be purchased at
An excellent interview of Dr Spector with Dana Parish was published in the Huffington Post below is an extract from that interview. The whole interview can be read –
Do you feel that ruling out Lyme should be imperative before diagnosing a patient with an auto-immune disease like MS, Fibromyalgia, or Rheumatoid Arthritis?
Absolutely! And Alzheimer’s. Something has to trigger an autoimmune disease. It doesn’t matter if this occurs in one percent or seventy-eight percent of the patient population–to allow people to go down a path of progressive neurodegeneration when they could be treated is unconscionable.
You have famously compared cancer to Lyme. What are their similarities?
To me, Lyme is the infectious disease equivalent of cancer. We don’t talk about cancer as just one disease anymore, and we should stop talking about Lyme this way. There are so many strains and co-infections. When you’re bitten by a tick, you can get five or ten different infections at the same time.
I also find it ludicrous to call all tick-borne disease, Lyme Disease. In breast cancer, we don’t just say, “You have breast cancer,” because that simply doesn’t mean anything anymore. The language is important because it has a bearing on treatment.
With cancer, we know that administering one algorithmic form of treatment doesn’t work. You have to understand the wiring that drives those tumors–the nuances, the mutations–and target them specifically. I think we need to start thinking this way about
Below are further links:-